Acoustic neuroma, also known as vestibular schwannoma, is a noncancerous and usually slow-growing tumor that develops on the main (vestibular) nerve leading from your inner ear to your brain. Branches of this nerve directly influence your balance and hearing, and pressure from an acoustic neuroma can cause hearing loss, ringing in your ear and unsteadiness.
Acoustic neuroma usually arises from the Schwann cells covering this nerve and grows slowly or not at all. Rarely, it may grow rapidly and become large enough to press against the brain and interfere with vital functions.
Treatments for acoustic neuroma include regular monitoring, radiation and surgical removal.
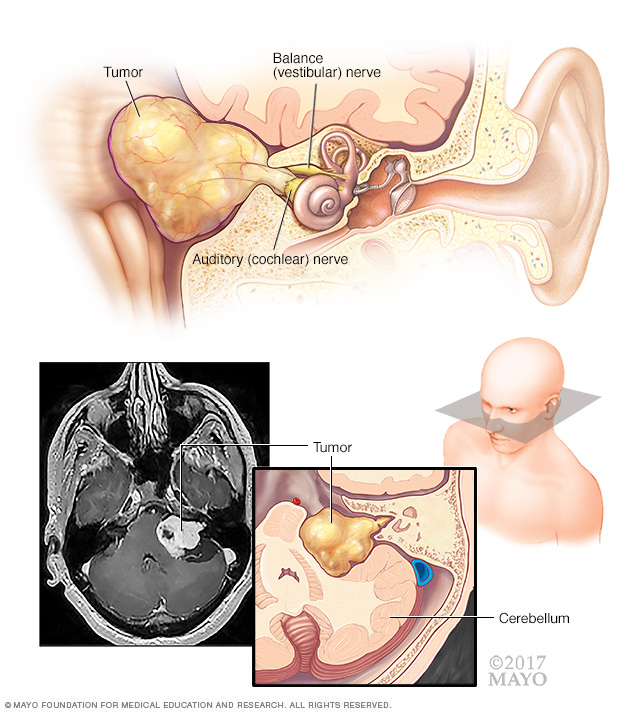
An acoustic neuroma (vestibular schwannoma) is a benign tumor that develops on the balance (vestibular) and hearing, or auditory (cochlear) nerves leading from your inner ear to the brain, as shown in the top image. The pressure on the nerve from the tumor may cause hearing loss and imbalance. In some cases, the tumor may grow and affect the cerebellum or other brain tissues, as shown in the magnetic resonance imaging (MRI) scan and illustrations above.
Symptoms
Signs and symptoms of acoustic neuroma are often easy to miss and may take many years to develop. They usually happen because of the tumor's effects on the hearing and balance nerves. Pressure from the tumor on nearby nerves controlling facial muscles and sensation (facial and trigeminal nerves), nearby blood vessels, or brain structures may also cause problems.
As the tumor grows, it may cause more noticeable or severe signs and symptoms.
Common signs and symptoms of acoustic neuroma include:
- Hearing loss, usually gradually worsening over months to years — although in rare cases sudden — and occurring on only one side or more severe on one side
- Ringing (tinnitus) in the affected ear
- Unsteadiness or loss of balance
- Dizziness (vertigo)
- Facial numbness and weakness or loss of muscle movement
In rare cases, an acoustic neuroma may grow large enough to compress the brainstem and become life-threatening.
When to see your doctor
See your doctor if you notice hearing loss in one ear, ringing in your ear or trouble with your balance.
Early diagnosis of an acoustic neuroma may help keep the tumor from growing large enough to cause serious consequences, such as total hearing loss.
Causes
The cause of acoustic neuromas can be linked to a problem with a gene on chromosome 22. Normally, this gene produces a tumor suppressor protein that helps control the growth of Schwann cells covering the nerves.
Experts don't know what causes this problem with the gene. In most cases of acoustic neuroma, there is no known cause. This faulty gene is also inherited in neurofibromatosis type 2, a rare disorder that usually involves the growth of tumors on the hearing and balance nerves on both sides of your head (bilateral vestibular schwannomas).
Risk factors
Neurofibromatosis type 2
The only confirmed risk factor for acoustic neuroma is having a parent with the rare genetic disorder neurofibromatosis type 2. However, neurofibromatosis type 2 only accounts for about 5% of acoustic neuroma cases.
A hallmark characteristic of neurofibromatosis type 2 is the development of noncancerous tumors on the hearing and balance nerves on both sides of the head, as well as on other nerves.
Neurofibromatosis type 2 (NF2) is known as an autosomal dominant disorder, meaning that the mutation can be passed on by just one parent (dominant gene). Each child of an affected parent has a 50-50 chance of inheriting it.
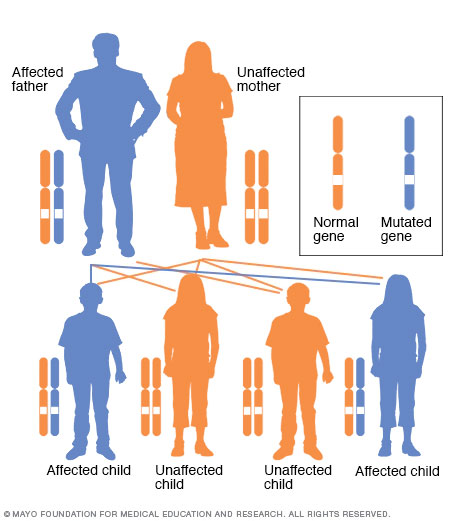
In an autosomal dominant disorder, the altered gene is a dominant gene located on one of the nonsex chromosomes (autosomes). You need only one altered gene to be affected by this type of disorder. A person with an autosomal dominant disorder — in this case, the father — has a 50% chance of having an affected child with one altered gene (dominant gene) and a 50% chance of having an unaffected child with two typical genes (recessive genes).
Complications
An acoustic neuroma may cause a variety of permanent complications, including:
- Hearing loss
- Facial numbness and weakness
- Difficulties with balance
- Ringing in the ear
Large tumors may press on your brainstem, preventing the normal flow of fluid between your brain and spinal cord (cerebrospinal fluid). In this case, fluid can build up in your head (hydrocephalus), increasing the pressure inside your skull.
Diagnosis
Acoustic neuroma is often difficult to diagnose in the early stages because signs and symptoms may be easy to miss and develop slowly over time. Common symptoms such as hearing loss are also associated with many other middle and inner ear problems.
After asking questions about your symptoms, your doctor will conduct an ear exam. Your doctor may order the following tests:
-
Hearing test (audiometry). In this test, conducted by a hearing specialist (audiologist), you hear sounds directed to one ear at a time. The audiologist presents a range of sounds of various tones and asks you to indicate each time you hear the sound. Each tone is repeated at faint levels to find out when you can barely hear.
The audiologist may also present various words to determine your hearing ability.
- Imaging. Magnetic resonance imaging (MRI) with contrast dye is usually used to diagnose acoustic neuroma. This imaging test can detect tumors as small as 1 to 2 millimeters in diameter. If MRI is unavailable or you can't have an MRI scan for some reason, computerized tomography (CT) may be used. However, CT scans may miss very small tumors.
Treatment
Your acoustic neuroma treatment may vary, depending on:
- The size and growth of the acoustic neuroma
- Your overall health
- Severity of symptoms
To treat acoustic neuroma, your doctor may suggest one or more of three potential options: monitoring, surgery or radiation therapy.
Monitoring
If you have a small acoustic neuroma that isn't growing or is growing slowly and causes few or no signs or symptoms, you and your doctor may decide to monitor it. Monitoring may be recommended if you're an older adult or otherwise not a good candidate for more-aggressive treatment.
Your doctor may recommend that you have regular imaging and hearing tests, usually every 6 to 12 months, to determine whether the tumor is growing and how quickly. If the scans show the tumor is growing or if the tumor causes progressive symptoms or other difficulties, you may need to undergo treatment.
Surgery
You may need surgery to remove an acoustic neuroma, especially if the tumor is:
- Continuing to grow
- Very large
- Causing symptoms
Your surgeon may use one of several techniques for removing an acoustic neuroma, depending on the size of your tumor, hearing status and other factors.
The goal of surgery is to remove the tumor and preserve the facial nerve to prevent facial paralysis. Removing the entire tumor may not be possible in certain cases — for example, if the tumor is too close to important parts of the brain or the facial nerve.
Surgery for an acoustic neuroma is performed under general anesthesia and involves removing the tumor through the inner ear or through a window in your skull.
Sometimes, surgical removal of the tumor may worsen symptoms if the hearing, balance, or facial nerves are irritated or damaged during the operation. Hearing may be lost on the side where the surgery is performed, and balance is usually affected temporarily.
Complications may include:
- Leaking cerebrospinal fluid through the wound or nose
- Hearing loss
- Facial weakness or numbness
- Ringing in the ear
- Balance problems
- Persistent headache
- Rarely, infection of the cerebrospinal fluid (meningitis)
- Very rarely, stroke or brain bleeding
Radiation therapy
There are several types of radiation therapy used to treat acoustic neuroma:
-
Stereotactic radiosurgery. Your doctor may recommend a type of radiation therapy known as stereotactic radiosurgery. It's often used if your tumor is small (less than 2.5 centimeters in diameter), you are an older adult or you cannot tolerate surgery for health reasons.
Stereotactic radiosurgery, such as Gamma Knife radiosurgery, uses many tiny gamma rays to deliver a precisely targeted dose of radiation to a tumor without damaging the surrounding tissue or making an incision.
The goal of stereotactic radiosurgery is to stop the growth of a tumor, preserve the facial nerve's function and possibly preserve hearing.
It may take weeks, months or years before you notice the effects of radiosurgery. Your doctor will monitor your progress with follow-up imaging studies and hearing tests.
Risks of radiosurgery include:
- Hearing loss
- Ringing in the ear
- Facial weakness or numbness
- Balance problems
- Continued tumor growth
- Stereotactic radiotherapy. Fractionated stereotactic radiotherapy (SRT) delivers a small dose of radiation to the tumor over several sessions. SRT is done to curb the growth of the tumor without damaging surrounding brain tissue.
- Proton beam therapy. This type of radiation therapy uses high-energy beams of positively charged particles called protons. Protons are delivered to the affected area in targeted doses to treat tumors and minimize radiation exposure to the surrounding area.
Supportive therapy
In addition to treatment to remove or stop the growth of the tumor, your doctor may recommend supportive therapies to address symptoms or complications of an acoustic neuroma and its treatment, such as dizziness or balance problems.
Cochlear implants or other treatments may also be recommended to treat hearing loss.
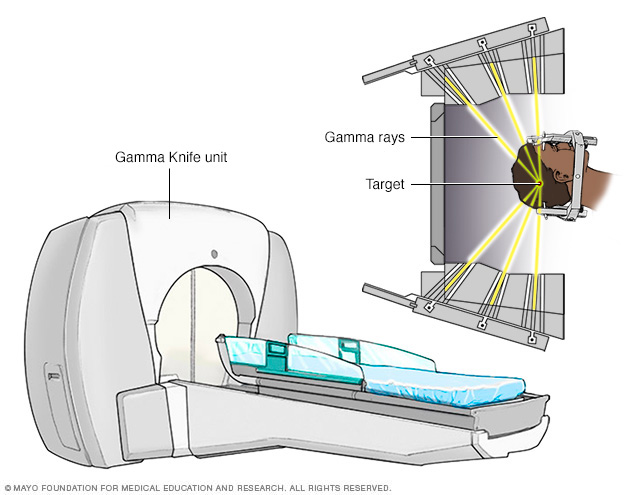
Gamma Knife stereotactic radiosurgery technology uses many small gamma rays to deliver a precise dose of radiation to a target.
Coping and support
Dealing with the possibility of hearing loss and facial paralysis and deciding which treatment would be best for you can be quite stressful. Here are some suggestions you may find helpful:
- Educate yourself about acoustic neuroma. The more you know, the better prepared you'll be to make good choices about treatment. Besides talking to your doctor and your audiologist, you may want to talk to a counselor or social worker. Or you may find it helpful to talk to other people who've had an acoustic neuroma and learn more about their experiences during and after treatment.
-
Maintain a strong support system. Family and friends can help you as you go through this difficult time. Sometimes, though, you may find the concern and understanding of other people with acoustic neuroma especially comforting.
Your doctor or a social worker may be able to put you in touch with a support group. Or you may find an in-person or online support group through the Acoustic Neuroma Association.
Preparing for an appointment
You're likely to start by seeing your family doctor or a general practitioner. Your doctor may then refer you to a doctor trained in ear, nose and throat conditions or a doctor trained in brain and nervous system surgery (neurosurgeon).
Because there's often a lot to talk about during your appointment, it's a good idea to be well prepared. Here's some information to help you get ready for your appointment, and what to expect from your doctor.
What you can do
- Write down any symptoms you're experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
- Make a list of all medications, vitamins or supplements that you're taking.
- Ask a family member or friend to join you, if possible. Sometimes it can be difficult to remember all the information provided to you during an appointment. Someone who accompanies you may remember something that you missed or forgot.
- Write down questions to ask your doctor.
Preparing a list of questions will help you make the most of your time with your doctor. For acoustic neuroma, some basic questions to ask your doctor include:
- What is likely causing my symptoms?
- Are there any other possible causes for my symptoms?
- What kinds of tests do I need?
- What treatment options are available?
- Which one do you recommend for me?
- What is the likelihood of side effects from each treatment option?
- What happens if I do nothing?
- Are there any brochures or other printed material that I can take home with me? What websites do you recommend visiting?
In addition to the questions that you've prepared to ask your doctor, don't hesitate to ask questions during your appointment.
What you can expect from your doctor
Your doctor is likely to ask you a number of questions. Being ready to answer them may reserve time to go over any points you want to spend more time on. Your doctor may ask:
- When did you first begin experiencing symptoms?
- Have your symptoms been continuous or occasional?
- How severe are your symptoms?
- Do you have any family members with an acoustic neuroma?
- At its current level, do you feel the hearing in the affected ear is useful to you in any way? For example, can you use that ear on the telephone, or does that ear help you tell where sound is coming from?
- Do you have regular headaches currently or have you had them in the past?
Copyright © 1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved.