Hypertrophic cardiomyopathy (HCM) is a disease in which the heart muscle becomes thickened (hypertrophied). The thickened heart muscle can make it harder for the heart to pump blood.
Hypertrophic cardiomyopathy often goes undiagnosed because many people with the disease have few, if any, symptoms. However, in a small number of people with HCM, the thickened heart muscle can cause shortness of breath, chest pain or changes in the heart's electrical system, resulting in life-threatening irregular heart rhythms (arrhythmias) or sudden death.
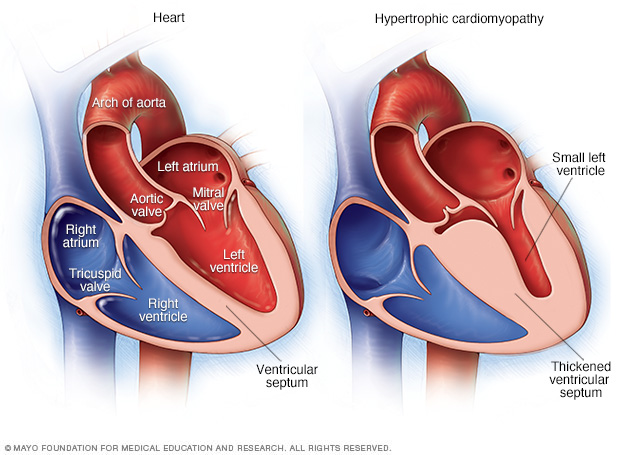
In hypertrophic cardiomyopathy (HCM), the muscular heart walls (septum) are much thicker (hypertrophied) than those in a typical heart. The thickening can occur anywhere in the left lower heart chamber (left ventricle).
Symptoms
Signs and symptoms of hypertrophic cardiomyopathy might include one or more of the following:
- Chest pain, especially during exercise
- Fainting, especially during or just after exercise or exertion
- Heart murmur, which a health care provider might detect while listening to the heart
- Sensation of fast, fluttering or pounding heartbeats (palpitations)
- Shortness of breath, especially during exercise
When to see a doctor
A number of conditions can cause shortness of breath and fast, pounding heartbeats. It's important to get a prompt, accurate diagnosis and appropriate care. See your health care provider if you have a family history of HCM or any symptoms associated with hypertrophic cardiomyopathy.
Call 911 or your local emergency number if you have any of the following symptoms for more than a few minutes:
- Rapid or irregular heartbeat
- Difficulty breathing
- Chest pain
Causes
Hypertrophic cardiomyopathy is usually caused by changes in genes (gene mutations) that cause the heart muscle to thicken.
Hypertrophic cardiomyopathy typically affects the muscular wall (septum) between the two bottom chambers of the heart (ventricles). The thickened wall might block blood flow out of the heart. This is called obstructive hypertrophic cardiomyopathy.
If there's no significant blocking of blood flow, the condition is called nonobstructive hypertrophic cardiomyopathy. However, the heart's main pumping chamber (left ventricle) might stiffen. This makes it hard for the heart to relax and reduces the amount of blood the ventricle can hold and send to the body with each heartbeat.
People with hypertrophic cardiomyopathy also have a rearrangement of heart muscle cells (myofiber disarray). This can trigger arrhythmias in some people.
Risk factors
Hypertrophic cardiomyopathy is usually passed down through families (inherited). People with one parent with hypertrophic cardiomyopathy have a 50% chance of having the genetic mutation for the disease.
Parents, children or siblings of a person with hypertrophic cardiomyopathy should ask their health care providers about screening for the disease.
Complications
Complications of hypertrophic cardiomyopathy can include:
- Atrial fibrillation. A thickened heart muscle and changes in the structure of heart cells can cause changes in the heart's electrical system, resulting in fast or irregular heartbeats. Atrial fibrillation can also increase the risk of developing blood clots, which can travel to the brain and cause a stroke.
- Blocked blood flow. In many people, the thickened heart muscle blocks the blood flow leaving the heart, causing shortness of breath with exertion, chest pain, dizziness and fainting spells.
- Mitral valve disease. If the thickened heart muscle blocks the blood flow leaving the heart, the valve between the left atrium and left ventricle (mitral valve) might not close properly. As a result, blood can leak backward into the left atrium (mitral valve regurgitation), possibly making symptoms worse.
- Dilated cardiomyopathy. In a small number of people with HCM, the thickened heart muscle becomes weak and ineffective. The ventricle becomes enlarged (dilated), and it pumps less forcefully.
- Heart failure. The thickened heart muscle can eventually become too stiff to fill the heart with blood. As a result, the heart can't pump enough blood to meet the body's needs.
- Fainting (syncope). An irregular heartbeat or blockage of blood flow can sometimes cause fainting. Unexplained fainting can be related to sudden cardiac death, especially if it's happened recently and in a young person.
- Sudden cardiac death. Rarely, hypertrophic cardiomyopathy can cause heart-related sudden death in people of all ages. Because many people with hypertrophic cardiomyopathy don't realize they have it, sudden cardiac death might be the first sign of the condition. It can happen in seemingly healthy young people, including high school athletes and other young, active adults.
Prevention
There is no known prevention for hypertrophic cardiomyopathy. It's important to identify the condition as early as possible to guide treatment and prevent complications.
If you have a first-degree relative — a parent, sibling or child — with hypertrophic cardiomyopathy, you might be referred for genetic testing to screen for the condition. However, not everyone with HCM has a currently detectable mutation. Also, some insurance companies don't cover genetic testing.
If genetic testing isn't done, or if the results aren't helpful, then a health care provider might recommend repeated echocardiograms if you have a family member with hypertrophic cardiomyopathy. Adolescents and competitive athletes should be screened once a year. Adults who don't compete in athletics should be screened every five years.
Diagnosis
Your health care provider will examine you and ask questions about your signs, symptoms, and medical and family history.
Tests
Your provider will likely order tests to diagnose hypertrophic cardiomyopathy (HCM) or rule out other conditions that can cause similar symptoms.
- Echocardiogram. An echocardiogram is commonly used to diagnose hypertrophic cardiomyopathy. This test uses sound waves (ultrasound) to see if the heart's muscle is unusually thick. It also shows how well the heart's chambers and valves are pumping blood.
-
Electrocardiogram (ECG or EKG). Sensors (electrodes) attached to adhesive pads are placed on the chest and sometimes the legs to measure electrical signals from the heart. An ECG can show irregular heart rhythms and signs of heart thickening.
Your health care provider may recommend monitoring your heartbeat at home. A portable ECG device (Holter monitor) can be worn for a day or more to record the heart's activity during daily activities.
- Cardiac MRI. This test uses powerful magnets and radio waves to create images of the heart. It provides information about the heart muscle and how the heart and heart valves work. This test is often done with an echocardiogram.
- Stress test. A stress test often involves walking on a treadmill or riding a stationary bike while the heart is monitored. Exercise stress tests help reveal how the heart responds to physical activity.
Treatment
The goals of hypertrophic cardiomyopathy treatment are to relieve symptoms and prevent sudden cardiac death in people at high risk. Treatment depends on the severity of symptoms. You and your health care provider will discuss the most appropriate treatment for your condition.
If you have cardiomyopathy and are pregnant or thinking about pregnancy, your health care provider might recommend that you see a doctor experienced in caring for women with high-risk pregnancies (perinatologist or maternal-fetal medicine specialist).
Medications
Medications can help reduce how strongly the heart muscle squeezes and slow the heart rate so that the heart can pump blood better. Medications to treat hypertrophic cardiomyopathy and its symptoms might include:
- Beta blockers such as metoprolol (Lopressor, Toprol-XL), propranolol (Inderal, Innopran XL) or atenolol (Tenormin)
- Calcium channel blockers such as verapamil (Verelan, Calan SR,) or diltiazem (Cardizem, Tiazac)
- Heart rhythm drugs such as amiodarone (Pacerone) or disopyramide (Norpace)
- Blood thinners such as warfarin (Jantoven), dabigatran (Pradaxa), rivaroxaban (Xarelto) or apixaban (Eliquis) to prevent blood clots if you have atrial fibrillation or the apical type of hypertrophic cardiomyopathy, which can increase the risk of sudden cardiac death.
Surgeries or other procedures
Several surgeries or procedures are available to treat cardiomyopathy or its symptoms. They include:
-
Septal myectomy. This open-heart surgery might be recommended if medications don't improve symptoms. It involves removing part of the thickened, overgrown wall (septum) between the heart chambers. Septal myectomy helps improve blood flow out of the heart and reduces backward flow of blood through the mitral valve (mitral regurgitation).
The surgery can be done using different approaches, depending on the location of the thickened heart muscle. In one type, called apical myectomy, surgeons remove thickened heart muscle from near the tip of the heart. Sometimes the mitral valve is repaired at the same time.
- Septal ablation. This procedure destroys the thickened heart muscle with alcohol. The alcohol is injected through a long, thin tube (catheter) into the artery supplying blood to that area. Possible complications include disruption of the heart's electrical system (heart block), which requires implantation of a pacemaker.
- Implantable cardioverter-defibrillator (ICD). An ICD is a small device that continuously monitors the heartbeat. It's implanted in the chest like a pacemaker. If a life-threatening arrhythmia occurs, the ICD delivers precisely calibrated electrical shocks to restore the heart rhythm. Use of an ICD has been shown to help prevent sudden cardiac death, which occurs in a small number of people with hypertrophic cardiomyopathy.
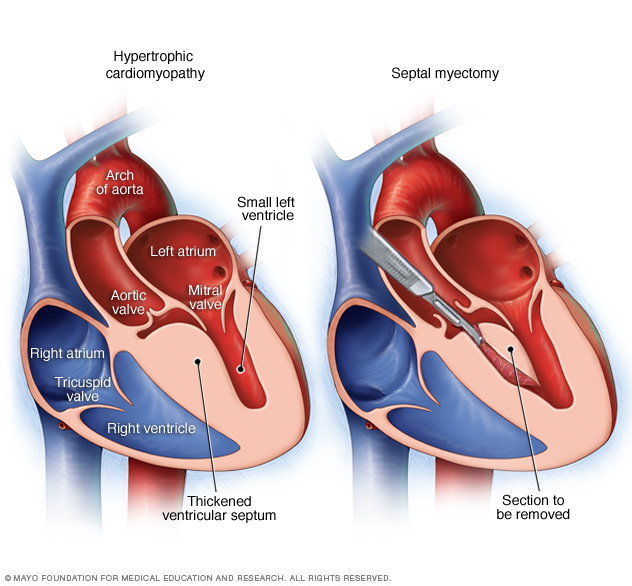
A septal myectomy is an open-heart procedure in which the surgeon removes part of the thickened, overgrown septum between the ventricles, as shown in the heart on the right.
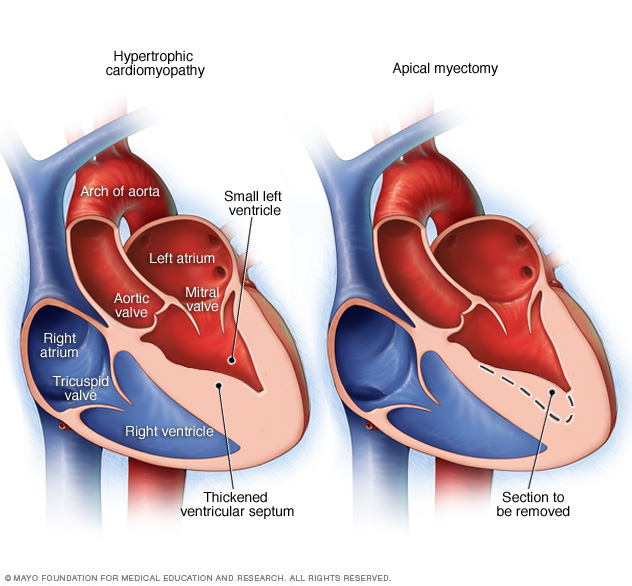
A septal myectomy is an open-heart procedure in which the surgeon removes part of the thickened, overgrown septum between the ventricles. In a type called apical myectomy, the thickened area is removed from the area near the tip of the heart.
Lifestyle and home remedies
Lifestyle changes, such as the following, can reduce the risk of complications related to hypertrophic cardiomyopathy.
- Exercising. You'll likely be able to engage in moderate-intensity exercise as part of a healthy lifestyle. If you want more-vigorous exercise, talk to your health care provider about your potential risks.
- Eating a healthy diet. A healthy diet is an important part of maintaining heart health.
- Maintaining a healthy weight. Maintaining a healthy weight will prevent excessive stress on the heart and reduce health risks associated with surgery or other procedures.
- Limit or avoid alcohol. In some cases, irregular heart rhythms and blocked blood flow are triggered or worsened by alcohol use. Ask your health care provider how much alcohol, if any, is safe for you to drink. If you choose to drink alcohol, do so in moderation. For healthy adults, that means up to one drink a day for women and up to two drinks a day for men.
- Having regular medical appointments. Your health care provider might recommend regular follow-up appointments to evaluate your condition. Let your provider know if you develop new or worse symptoms.
Coping and support
Being diagnosed with hypertrophic cardiomyopathy can cause a range of difficult emotions. Feelings of grief, fear and anger aren't uncommon.
To better manage your condition:
- Manage stress. Find ways to help reduce emotional stress. Getting more exercise and practicing mindfulness are ways to reduce stress.
- Seek support. Consider joining a support group. Support groups allow you to connect with others who have similar experiences.
Preparing for an appointment
You may be referred to a doctor trained in diagnosing and treating heart conditions (cardiologist). Here's some information to help you prepare for your appointment.
What you can do
When you make the appointment, ask about pre-appointment restrictions, such as changing your activity level or your diet. Make a list of:
- Your symptoms and when they began
- All medications, vitamins and supplements you take, including doses
- Key medical information, including other diagnosed conditions and family history of heart disease
- Questions to ask your health care provider
Questions to ask your health care provider might include:
- What's the most likely cause of my symptoms?
- What tests do I need?
- What treatments can help?
- What risks does my heart condition create?
- How often will I need follow-up appointments?
- Do I need to restrict my activities?
- Should my children or other first-degree relatives be screened for this condition, and should I meet with a genetic counselor?
- How will other conditions that I have or medications I take affect my heart condition?
Don't hesitate to ask other questions you have.
What to expect from your doctor
Your health care provider is likely to ask you a number of questions, such as:
- How severe are your symptoms?
- Have your symptoms changed over time? If so, how?
- Does exercise or physical exertion make your symptoms worse?
- Have you ever fainted?
What you can do in the meantime
Before your appointment, ask your family members if any relatives have been diagnosed with hypertrophic cardiomyopathy or have had unexplained, sudden death.
If exercise makes your symptoms worse, avoid strenuous exercise until you have seen your health care provider and received specific exercise recommendations.
Copyright © 1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved.