Boxed Warning
Cardiovascular disorders (tablet):
Estrogen plus progestin therapy should not be used for the prevention of cardiovascular disease. The Women's Health Initiative (WHI) estrogen plus progestin substudy reported increased risks of deep vein thrombosis (DVT), pulmonary embolism (PE), stroke, and myocardial infarction (MI) in postmenopausal women (50 to 79 years of age) during 5.6 years of treatment with daily oral conjugated estrogens (0.625 mg) combined with medroxyprogesterone acetate (2.5 mg), relative to placebo.
Breast cancer (tablet):
The Women's Health Initiative (WHI) estrogen plus progestin substudy demonstrated an increased risk of invasive breast cancer.
Dementia (tablet):
Estrogen plus progestin therapy should not be used for the prevention of dementia. The Women's Health Initiative Memory Study (WHIMS) estrogen plus progestin ancillary study of the WHI reported an increased risk of developing probable dementia in postmenopausal women 65 years or older during 4 years of treatment with daily conjugated estrogens (0.625 mg) combined with medroxyprogesterone acetate (2.5 mg), relative to placebo. It is unknown whether this finding applies to younger postmenopausal women.
Long-term use (injection):
Medroxyprogesterone contraceptive should not be used as a long-term birth control method (ie, longer than 2 years) unless other birth control methods are considered inadequate.
Loss of bone mineral density (injection):
Women who use medroxyprogesterone contraceptive may lose significant bone mineral density (BMD). Bone loss is greater with increasing duration of use and may not be completely reversible. It is unknown if use of medroxyprogesterone contraceptive during adolescence or early adulthood, a critical period of bone accretion, will reduce peak bone mass and increase the risk for osteoporotic fracture in later life.
Patient education (subcutaneous injection):
Patients should be counseled that medroxyprogesterone contraceptive does not protect against HIV infection (AIDS) and other sexually transmitted diseases.
Risk vs benefits (tablet):
In the absence of comparable data, these risks should be assumed to be similar for other doses of conjugated estrogens and medroxyprogesterone acetate, and other combinations and dosage forms of estrogens and progestins. Estrogens with progestins should be prescribed at the lowest effective doses and for the shortest duration consistent with treatment goals and risks for the individual woman.
Dosage Forms
Excipient information presented when available (limited, particularly for generics); consult specific product labeling. [DSC] = Discontinued product
Suspension, Intramuscular, as acetate:
Depo-Provera: 150 mg/mL (1 mL) [contains methylparaben, polyethylene glycol, polysorbate 80, propylparaben]
Depo-Provera: 400 mg/mL (2.5 mL) [contains polyethylene glycol]
Generic: 150 mg/mL (1 mL)
Suspension Prefilled Syringe, Intramuscular, as acetate:
Depo-Provera: 150 mg/mL (1 mL) [contains methylparaben, polyethylene glycol, polysorbate 80, propylparaben]
Generic: 150 mg/mL (1 mL)
Suspension Prefilled Syringe, Subcutaneous, as acetate:
Depo-SubQ Provera 104: 104 mg/0.65 mL (0.65 mL) [contains methylparaben, polyethylene glycol, polysorbate 80, propylparaben]
Tablet, Oral, as acetate:
Provera: 2.5 mg, 5 mg [DSC] [scored]
Provera: 5 mg [contains corn starch, fd&c blue #2 aluminum lake]
Provera: 10 mg [scored]
Generic: 2.5 mg, 5 mg, 10 mg
Pharmacology
Mechanism of Action
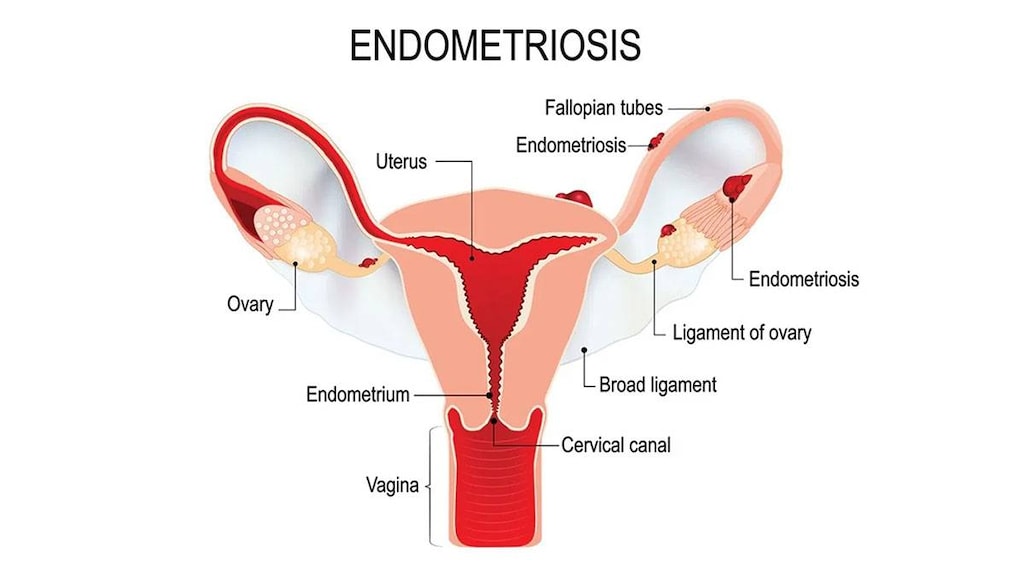
Medroxyprogesterone acetate (MPA) transforms a proliferative endometrium into a secretory endometrium. When administered with conjugated estrogens, MPA reduces the incidence of endometrial hyperplasia and risk of adenocarcinoma. When used as an injection for contraception (doses of 150 mg IM or 104 mg SubQ), MPA inhibits secretion of pituitary gonadotropins, which prevents follicular maturation and ovulation and causes endometrial thinning. Progestogens, such as medroxyprogesterone when used for endometriosis, lead to atrophy of the endometrial tissue. They may also suppress new growth and implantation. Pain associated with endometriosis is decreased (ASRM 2014).
Pharmacokinetics/Pharmacodynamics
Absorption
Oral: Rapid; IM: Slow
Metabolism
Extensively hepatic via hydroxylation and conjugation; forms metabolites
Excretion
Urine
Onset of Action
Time to ovulation (after last injection): 10 months (range: 6 to 12 months)
Time to Peak
Oral: 2 to 4 hours; IM (Depo-Provera Contraceptive): ~3 weeks; SubQ: ~1 week
Half-Life Elimination
Oral: 12 to 17 hours; IM (Depo-Provera Contraceptive): ~50 days; SubQ: ~43 days
Protein Binding
86% to 90% primarily to albumin; does not bind to sex hormone-binding globulin
Use: Labeled Indications
Abnormal uterine bleeding (tablet): Treatment of abnormal uterine bleeding due to hormonal imbalance in the absence of organic pathology, such as fibroids or uterine cancer.
Amenorrhea, secondary (tablet): Treatment of secondary amenorrhea due to hormonal imbalance in the absence of organic pathology, such as fibroids or uterine cancer.
Contraception (104 mg/0.65 mL and 150 mg/mL injection): Prevention of pregnancy in women of childbearing potential.
Endometrial hyperplasia prevention (tablet): Prevention of endometrial hyperplasia in nonhysterectomized postmenopausal persons receiving daily oral conjugated estrogens 0.625 mg. Note: Due to safety considerations, when a progesterone is needed, use of micronized progesterone is preferred over medroxyprogesterone acetate (AACE [Goodman 2011]; AACE/ACE [Cobin 2017])
Endometrial carcinoma (400 mg/mL injection) (100 mg tablet [Canadian product]): Adjunctive therapy and/or palliative treatment of inoperable, recurrent, and/or metastatic endometrial carcinoma.
Endometriosis (104 mg/0.65 mL injection): Management of endometriosis-associated pain.
Use: Off Label
Abnormal uterine bleeding, acutebyes
Data from a randomized, open-label clinical study support the use of oral medroxyprogesterone in the treatment of acute uterine bleeding in nonpregnant, hemodynamically stable premenopausal women requiring emergent medical intervention Munro 2006.
Based on the American College of Obstetricians and Gynecologists (ACOG) committee opinion on the management of acute abnormal uterine bleeding in nonpregnant reproductive-aged women, medroxyprogesterone is effective and recommended for the management of acute abnormal uterine bleeding in patients who are clinically stable ACOG 557 2013.
Endometrial hyperplasia (treatment)byes
Data from a randomized study comparing levonorgestrel IUD and oral medroxyprogesterone (cyclical and continuous dosing) demonstrated the efficacy of both continuous dosing medroxyprogesterone and levonorgestrel IUD for the treatment of low- and medium-risk endometrial hyperplasia Orbo 2014. Clinical experience also suggests the utility of medroxyprogesterone for non-surgical management of endometrial hyperplasia (with or without atypia) or endometrial precancers; the specific dose, route of administration, and duration are dependent on the diagnosis as well as patient specific factors Armstrong 2012, Trimble 2012. Findings from a systematic review indicate that levonorgestrel IUD may be preferred over oral progestins in the treatment of non-atypical endometrial hyperplasia Abu Hashim 2016.
According to the ACOG committee opinion paper on endometrial intraepithelial neoplasia (formerly called atypical endometrial hyperplasia), medroxyprogesterone is one progestin that may be used in the nonsurgical management of endometrial precancers in patients who desire future fertility or who are not candidates for surgery ACOG 631 2015.
Hot flashes (intramuscular administration)b
Data support the efficacy of medroxyprogesterone for reduction of hot flash frequency and/or severity, which relates directly to an improvement in quality of life for women with natural or medically induced menopause.Loprinzi 2006, Loprinzi 2008
Paraphilia/hypersexuality (treatment)c
Clinical experience suggests the utility of medroxyprogesterone in the treatment of paraphilia/hypersexuality Reilly 2000. Additional data may be necessary to further define the role of medroxyprogesterone in the management of this condition.
Contraindications
Injection (104 mg/0.65 mL): Hypersensitivity to medroxyprogesterone or any component of the formulation; active thrombophlebitis; thromboembolic disorders (current or history of); cerebral vascular disease; undiagnosed vaginal bleeding; breast cancer (known, suspected, or history of); significant hepatic disease; pregnancy
Injection (150 mg/mL): Hypersensitivity to medroxyprogesterone or any component of the formulation; active thrombophlebitis; thromboembolic disorders (current or history of) or cerebral vascular disease; undiagnosed vaginal bleeding; breast cancer (known, suspected, or history of); significant hepatic disease; pregnancy; diagnostic test for pregnancy
Injection (400 mg/mL): Hypersensitivity to medroxyprogesterone or any component of the formulation; active thrombophlebitis; thromboembolic disorders (current or history of); cerebral vascular disease
Tablet: Anaphylactic reaction or angioedema to medroxyprogesterone; DVT or PE (current or history of); active or history of arterial thromboembolic disease (eg, stroke, MI); estrogen- or progesterone-dependent tumor (known or suspected) (excludes 100 mg tablet [Canadian product] indicated for endometrial cancer); undiagnosed abnormal genital bleeding; breast cancer (known, suspected, or history of); hepatic impairment or disease; pregnancy
Canadian labeling: Additional contraindications (not in the US labeling):
Injection (50 mg/mL, 104 mg per 0.65 mL, 150 mg/mL): History of or current benign or malignant liver tumors; current or history of migraine with focal aura; any ocular lesion arising from ophthalmic vascular disease, such as partial or complete loss of vision or defect in visual fields; undiagnosed breast pathology; known or suspected progestin-dependent neoplasia; MI or coronary artery disease (current or history of); urinary tract bleeding; presence of severe or multiple risk factors for arterial or venous thrombosis including the following: severe hypertension (persistent bp ≥160/100 mm Hg); hereditary or acquired predisposition for venous or arterial thrombosis (eg, Factor V leiden and Prothrombin G20210 A mutation, activated protein C (APC) resistance, antithrombin-III-deficiency, protein C deficiency, protein S deficiency, hyperhomocysteinanemia and antiphospholipid-antibodies (anticardiolipin antibodies, lupus anticoagulant); severe dyslipoproteinemia; heavy smoking (>15 cigarettes per day) and older than 35 years of age; diabetes mellitus with vascular involvement
Tablet: Partial or complete loss of vision due to ophthalmic vascular disease
Dosage and Administration
Dosing: Adult
Abnormal uterine bleeding: Oral: 5 or 10 mg daily for 5 to 10 days starting on day 16 or 21 of menstrual cycle. A suggested dose of 10 mg daily for 10 days starting on day 16 of the cycle induces optimum secretory transformation of the endometrium when adequately primed with endogenous or exogenous estrogen. Withdrawal bleeding may be expected within 3 to 7 days after discontinuing medroxyprogesterone. Planned menstrual cycling may benefit patients with a history of recurrent episodes of abnormal uterine bleeding.
Abnormal uterine bleeding, acute (off-label): Oral: 20 mg three times a day for 7 days (ACOG 557 2013; Munro 2006)
Amenorrhea, secondary: Oral: 5 or 10 mg daily for 5 to 10 days. Therapy may be started at any time. A dose of 10 mg daily for 10 days induces optimum secretory transformation of the endometrium when adequately primed with endogenous or exogenous estrogen. Withdrawal bleeding may be expected within 3 to 7 days after discontinuing
Contraception:
Depo-Provera Contraceptive: IM: 150 mg every 3 months (every 13 weeks)
Depo-subQ Provera 104: SubQ: 104 mg every 3 months (every 12 to 14 weeks)
Endometrial carcinoma, recurrent or metastatic (adjunctive/palliative treatment):
IM (Depo-Provera): Initial: 400 to 1,000 mg/week
Oral (100 mg tablet [Canadian product]): Manufacturer’s labeling: Usual dose: 200 to 400 mg daily. Doses >200 mg daily may not confer additional benefit (Thigpen 1999). If improvement or disease stabilization occurs, 200 mg daily may be sufficient for maintenance. Discontinue use if no improvement within 2 to 3 months.
Endometrial hyperplasia prevention in postmenopausal persons receiving daily conjugated estrogen (alternative agent): Oral: 5 or 10 mg daily for 12 to 14 consecutive days each month, starting on day 1 or day 16 of the cycle. When treating postmenopausal persons, use for the shortest duration possible at the lowest effective dose consistent with treatment goals. Reevaluate patients as clinically appropriate to determine if treatment is still necessary. Treatment is indicated for postmenopausal persons with a uterus to decrease the risk of endometrial cancer; persons who have had a hysterectomy generally do not need a progestin. Due to safety considerations, when a progesterone is needed, use of micronized progesterone is preferred over medroxyprogesterone acetate (AACE [Goodman 2011]; AACE/ACE [Cobin 2017]; Goodman [AACE] 2011).
Endometrial hyperplasia, treatment (off-label use): Note: The optimal duration of therapy is unknown (ACOG 631 2015; Armstrong 2012; Trimble 2012).
Atypical endometrial hyperplasia or endometrial intraepithelial neoplasia: Oral: 10 to 20 mg once daily (continuous dosing) or 10 mg to 20 mg once daily (cyclic dosing) for 12 to 14 days per month (ACOG 631 2015; Trimble 2012).
Non-atypical hyperplasia: Oral: 10 mg once daily (continuous dosing) (Orbo 2014) or 10 mg once daily (cyclic dosing) for 10 to 12 days per cycle (Abu Hashim 2016); continuous daily oral dosing was shown to be superior to cyclic oral dosing (Orbo 2014).
Endometriosis (Depo-subQ Provera 104): SubQ: 104 mg every 3 months (every 12 to 14 weeks)
Hot flashes (off-label use): IM: 400 mg as single dose (Loprinzi 2006)
Paraphilia/hypersexuality (off-label use) (Reilly 2000): Males (Note: Avoid use if active pituitary pathology, hepatic failure, or thromboembolic disease):
IM (Depo-Provera): 100 to 600 mg weekly
Oral: 100 to 500 mg daily
Dosing: Geriatric
Refer to adult dosing.
Dosing: Pediatric
Abnormal uterine bleeding: Adolescents: Oral: 5 to 10 mg for 5 to 10 days starting on day 16 or day 21 of menstrual cycle
Amenorrhea: Adolescents: Oral: 5 to 10 mg/day for 5 to 10 days
Contraception: Adolescents: First dose to be given only during first 5 days of normal menstrual period; only within 5 days postpartum if not breast-feeding, or only at sixth postpartum week if exclusively breast-feeding. When switching from other contraceptive methods, depo-subQ provera 104 should be administered within 7 days after the last day of using the last method (pill, ring, patch).
IM (Depo-Provera): 150 mg every 3 months (every 13 weeks)
SubQ (depo-subQ provera 104): 104 mg every 3 months (every 12 to 14 weeks)
Endometriosis-associated pain: Adolescents: SubQ (depo-subQ provera 104): 104 mg every 3 months; treatment longer than 2 years is not recommended due to impact of long-term use on bone mineral density
Administration
IM: Depo-Provera Contraceptive: Administer first dose during the first 5 days of menstrual period, or within the first 5 days postpartum if not breastfeeding, or at the sixth week postpartum if breastfeeding exclusively. Shake vigorously prior to administration. Administer by deep IM injection in the gluteal or deltoid muscle. Rotate administration site with each injection.
When switching from combined hormonal contraceptives (estrogen plus progestin), the first injection should be on the day after the last active tablet or (at the latest) the day after the final inactive tablet. When switching from other contraceptive methods, ensure continuous contraceptive coverage.
SubQ: Depo-subQ Provera 104: Administer first dose during the first 5 days of menstrual period, or at the sixth week postpartum if breastfeeding. Shake vigorously for at least 1 minute prior to administration. Administer by SubQ injection in the anterior thigh or abdomen; avoid boney areas and the umbilicus. Administer slowly over 5 to 7 seconds. Do not rub the injection area. Rotate administration site with each injection.
When switching from combined hormonal contraceptives (estrogen plus progestin), the first injection should be within 7 days after the last active pill, or removal of patch or ring. If switching from the IM to SubQ formulation, the next dose should be given within the prescribed dosing period for the IM injection to ensure continuous coverage.
IM, SubQ: Additional contraceptive considerations: Available guidelines note the first injection may be given at any time in the menstrual cycle once it is determined that the woman is not pregnant. Back-up contraception is not needed if given within 7 days of onset of menstruation, immediately postpartum, or immediately after a spontaneous or induced abortion. Additional contraception is needed for 7 days unless the injection is given at the time of a surgical abortion. If the injection is given >7 days after menstrual bleeding started, an additional form of contraception must be used for 7 days unless the woman abstains from sexual intercourse. When switching from an IUD to the injection in women who have had sexual intercourse since the start of their last menstrual cycle, consider postponing removal of the IUD for 7 days after the initial injection, instruct the woman to use barrier contraception or abstain from intercourse for 7 days before the first injection, or consider emergency contraception at the time of IUD removal. When contraception will be continued, repeat injections should be given every 13 weeks but may be given early if needed. Injections may be given up to 2 weeks late, however pregnancy should be ruled out and additional contraceptive measures are required for 7 days if the repeat dose is >15 weeks from the last injection (Curtis 2016a).
Dietary Considerations
Ensure adequate calcium and vitamin D intake
Storage
Store at 20°C to 25°C (68°F to 77°F).
MedroxyPROGESTERone Images


Drug Interactions
Acitretin: May diminish the therapeutic effect of Progestins (Contraceptive). Contraceptive failure is possible. Management: Given the potential for progestin-only preparations to fail to prevent pregnancy during acitretin therapy, such products should not be relied upon. Alternative, nonhormonal forms of contraception must be employed during acitretin therapy. Consider therapy modification
Anticoagulants: Progestins may diminish the therapeutic effect of Anticoagulants. More specifically, the potential prothrombotic effects of some progestins and progestin-estrogen combinations may counteract anticoagulant effects. Management: Carefully weigh the prospective benefits of progestins against the potential increased risk of procoagulant effects and thromboembolism. Use is considered contraindicated under some circumstances. Refer to related guidelines for specific recommendations. Consider therapy modification
Antidiabetic Agents: Hyperglycemia-Associated Agents may diminish the therapeutic effect of Antidiabetic Agents. Monitor therapy
Aprepitant: May decrease the serum concentration of Progestins (Contraceptive). Management: Alternative or additional methods of contraception should be used both during treatment with aprepitant or fosaprepitant and for at least one month following the last aprepitant/fosaprepitant dose. Consider therapy modification
Artemether: May decrease the serum concentration of Progestins (Contraceptive). Management: Consider the use of an alternative (i.e., non-hormonal) means of contraception in all women of childbearing potential who are using artemether. Consider therapy modification
Atazanavir: May increase the serum concentration of Progestins (Contraceptive). However, atazanavir may lead to decreased ethinyl estradiol concentrations and decreased effectiveness of oral contraceptive products. Management: Consider an alternative or additional method of contraception, particularly with combined estrogen/progestin products. Depot medroxyprogesterone acetate may be used without a need for additional contraception. Consider therapy modification
Barbiturates: May diminish the therapeutic effect of Progestins (Contraceptive). Contraceptive failure is possible. Management: Use of alternative, nonhormonal contraceptives is recommended. Consider therapy modification
Bexarotene (Systemic): May decrease the serum concentration of Progestins (Contraceptive). Management: Women of childbearing potential receiving bexarotene should use two reliable forms of contraception (including at least one nonhormonal form). Consider therapy modification
Bile Acid Sequestrants: May decrease the serum concentration of Progestins (Contraceptive). Management: Administer oral progestin-containing contraceptives at least 1 to 4 hours prior to or 4 to 6 hours after administration of a bile acid sequestrant. Consider therapy modification
Bosentan: May decrease the serum concentration of Progestins (Contraceptive). Management: Use an alternative (i.e., non-hormonal) means of contraception for all women of childbearing potential who are using bosentan, and do not rely on hormonal contraceptives alone. Consider therapy modification
Brigatinib: May decrease the serum concentration of Progestins (Contraceptive). Management: Females of childbearing potential should use an alternative, non-hormonal contraceptive during brigatinib therapy and for at least 4 months after the final brigatinib dose. Consider therapy modification
C1 inhibitors: Progestins may enhance the thrombogenic effect of C1 inhibitors. Monitor therapy
CarBAMazepine: May diminish the therapeutic effect of Progestins (Contraceptive). Contraceptive failure is possible. Management: Use of alternative, nonhormonal contraceptives is recommended. Consider therapy modification
Carfilzomib: May enhance the thrombogenic effect of Progestins (Contraceptive). Management: Consider alternative, non-hormonal methods of contraception in patients requiring therapy with carfilzomib. Consider therapy modification
Cenobamate: May decrease the serum concentration of Hormonal Contraceptives. Management: Women should use additional or alternative non-hormonal birth control while taking cenobamate. Consider therapy modification
Choline C 11: Antiandrogens may diminish the therapeutic effect of Choline C 11. Monitor therapy
Cladribine: May diminish the therapeutic effect of Hormonal Contraceptives. Management: Women using systemically acting hormonal contraceptives should add a barrier method during cladribine dosing and for at least 4 weeks after the last dose in each treatment course. Consider therapy modification
CloBAZam: May decrease the serum concentration of Progestins (Contraceptive). Consider therapy modification
Cobicistat: May increase the serum concentration of Progestins (Contraceptive). Management: Consider an alternative, nonhormone-based contraceptive in patients receiving cobicistat-containing products. Drospirenone is specifically contraindicated with atazanavir and cobicistat. Consider therapy modification
CYP3A4 Inducers (Moderate): May decrease the serum concentration of CYP3A4 Substrates (High risk with Inducers). Monitor therapy
CYP3A4 Inducers (Strong): May increase the metabolism of CYP3A4 Substrates (High risk with Inducers). Management: Consider an alternative for one of the interacting drugs. Some combinations may be specifically contraindicated. Consult appropriate manufacturer labeling. Consider therapy modification
CYP3A4 Inhibitors (Strong): May increase the serum concentration of MedroxyPROGESTERone. Exceptions: Atazanavir; Cobicistat; Darunavir; Lopinavir; Nelfinavir; Saquinavir. Monitor therapy
Dabrafenib: May decrease the serum concentration of CYP3A4 Substrates (High risk with Inducers). Management: Seek alternatives to the CYP3A4 substrate when possible. If concomitant therapy cannot be avoided, monitor clinical effects of the substrate closely (particularly therapeutic effects). Consider therapy modification
Dabrafenib: May decrease the serum concentration of Progestins (Contraceptive). Management: Females of reproductive potential should use an alternative, highly effective, non-hormonal means of contraception during and at least 2 weeks (dabrafenib alone) or 4 months (dabrafenib + trametinib) after discontinuation of dabrafenib treatment. Consider therapy modification
Darunavir: May decrease the serum concentration of Progestins (Contraceptive). Management: Consider using an alternative or additional means of contraception. Injected depot medroxyprogesterone acetate may be used without a need for additional contraception. Consider therapy modification
Deferasirox: May decrease the serum concentration of CYP3A4 Substrates (High risk with Inducers). Monitor therapy
Efavirenz: May decrease the serum concentration of Progestins (Contraceptive). Management: Use an alternative or additional method of contraception due to possibly decreased contraceptive effectiveness. Injected depot medroxyprogesterone acetate does not appear to participate in this interaction. Consider therapy modification
Elexacaftor, Tezacaftor, and Ivacaftor: Hormonal Contraceptives may enhance the adverse/toxic effect of Elexacaftor, Tezacaftor, and Ivacaftor. Specifically, the risk for rash may be increased. Monitor therapy
Encorafenib: May decrease the serum concentration of Progestins (Contraceptive). Avoid combination
Enzalutamide: May decrease the serum concentration of CYP3A4 Substrates (High risk with Inducers). Management: Concurrent use of enzalutamide with CYP3A4 substrates that have a narrow therapeutic index should be avoided. Use of enzalutamide and any other CYP3A4 substrate should be performed with caution and close monitoring. Consider therapy modification
Erdafitinib: May decrease the serum concentration of CYP3A4 Substrates (High risk with Inducers). Monitor therapy
Eslicarbazepine: May decrease the serum concentration of Progestins (Contraceptive). Management: Alternative, non-hormonal means of birth control should be considered for women of child-bearing potential. Consider therapy modification
Felbamate: May decrease the serum concentration of Progestins (Contraceptive). Management: Contraceptive failure is possible. Use of an alternative, nonhormonal method of contraception is recommended. Consider therapy modification
Flibanserin: Progestins (Contraceptive) may increase the serum concentration of Flibanserin. Monitor therapy
Fosamprenavir: Progestins (Contraceptive) may decrease serum concentrations of the active metabolite(s) of Fosamprenavir. Fosamprenavir may decrease the serum concentration of Progestins (Contraceptive). Management: Consider using an alternative or additional means of contraception. Injected depot medroxyprogesterone acetate may be used without a need for additional contraception. Consider therapy modification
Fosaprepitant: May decrease the serum concentration of Progestins (Contraceptive). The active metabolite aprepitant is likely responsible for this effect. Management: Alternative or additional methods of contraception should be used both during treatment with aprepitant or fosaprepitant and for at least one month following the last aprepitant/fosaprepitant dose. Consider therapy modification
Fosphenytoin: May diminish the therapeutic effect of Progestins (Contraceptive). Contraceptive failure is possible. Management: Contraceptive failure is possible. Use of an alternative, nonhormonal contraceptive is recommended. Consider therapy modification
Griseofulvin: May diminish the therapeutic effect of Progestins (Contraceptive). Contraceptive failure is possible. Avoid combination
Herbs (Progestogenic Properties) (eg, Bloodroot, Yucca): May enhance the adverse/toxic effect of Progestins. Monitor therapy
Indium 111 Capromab Pendetide: Antiandrogens may diminish the diagnostic effect of Indium 111 Capromab Pendetide. Avoid combination
Ivosidenib: May decrease the serum concentration of Progestins (Contraceptive). Management: Consider alternative methods of contraception (ie, non-hormonal) in patients receiving ivosidenib. Consider therapy modification
Ixazomib: May decrease the serum concentration of Progestins (Contraceptive). More specifically, use of ixazomib with dexamethasone may decrease the serum concentrations of contraceptive progestins. Management: Patients of childbearing potential should use a nonhormonal barrier contraceptive during and 90 days following ixazomib treatment. Avoid combination
LamoTRIgine: May decrease the serum concentration of Progestins (Contraceptive). Monitor therapy
Lesinurad: May decrease the serum concentration of Progestins (Contraceptive). Management: Use of an additional, nonhormonal contraceptive is recommended in patients being treated with lesinurad who desire effective contraception. Consider therapy modification
Lixisenatide: May decrease the serum concentration of Progestins (Contraceptive). Management: Administer oral contraceptives 1 hour before or at least 11 hours after administration of lixisenatide. Consider therapy modification
Lopinavir: May decrease the serum concentration of Progestins (Contraceptive). Lopinavir may increase the serum concentration of Progestins (Contraceptive). Management: Consider using an alternative or additional means of contraception. Injected depot medroxyprogesterone acetate and etonogestrel implants may be used without a need for additional contraception. Consider therapy modification
Lorlatinib: May decrease the serum concentration of CYP3A4 Substrates (High risk with Inducers). Management: Avoid concurrent use of lorlatinib with any CYP3A4 substrates for which a minimal decrease in serum concentrations of the CYP3A4 substrate could lead to therapeutic failure and serious clinical consequences. Consider therapy modification
Lumacaftor and Ivacaftor: May decrease the serum concentration of Hormonal Contraceptives. Management: Do not rely on hormone-based contraceptives with concurrent use of lumacaftor/ivacaftor; an alternative, non-hormonal, method of contraception should be used if this combination is required. Consider therapy modification
Metreleptin: May decrease the serum concentration of Progestins (Contraceptive). Metreleptin may increase the serum concentration of Progestins (Contraceptive). Monitor therapy
MiFEPRIStone: May diminish the therapeutic effect of Progestins (Contraceptive). MiFEPRIStone may increase the serum concentration of Progestins (Contraceptive). Management: Women of childbearing potential should use an effective, nonhormonal means of contraception during and 4 weeks following mifepristone treatment. Consider therapy modification
Mitotane: May decrease the serum concentration of CYP3A4 Substrates (High risk with Inducers). Management: Doses of CYP3A4 substrates may need to be adjusted substantially when used in patients being treated with mitotane. Consider therapy modification
Mycophenolate: May decrease the serum concentration of Progestins (Contraceptive). Management: Use of an additional or alternative (nonhormonal) method of contraception should be considered. Consider therapy modification
Nalmefene: MedroxyPROGESTERone may increase the serum concentration of Nalmefene. Monitor therapy
Nelfinavir: May decrease the serum concentration of Progestins (Contraceptive). Management: Use an alternative or additional method of contraception due to possibly decreased contraceptive effectiveness. Injected depot medroxyprogesterone acetate does not appear to participate in this interaction. Consider therapy modification
OXcarbazepine: May decrease the serum concentration of Progestins (Contraceptive). Management: Contraceptive failure is possible. Use of an additional or alternative, nonhormonal method of contraception is recommended. Consider therapy modification
Pegloticase: May diminish the therapeutic effect of PEGylated Drug Products. Monitor therapy
Pegvaliase: MedroxyPROGESTERone may enhance the adverse/toxic effect of Pegvaliase. Specifically, the risk of anaphylaxis or hypersensitivity reactions may be increased. Monitor therapy
Perampanel: May decrease the serum concentration of Progestins (Contraceptive). Management: Patients should use an alternative, nonhormonal-based form of contraception both during the concurrent use of perampanel and for 1 month after discontinuing perampanel. Consider therapy modification
Phenytoin: May diminish the therapeutic effect of Progestins (Contraceptive). Contraceptive failure is possible. Management: Contraceptive failure is possible. Use of an alternative, nonhormonal contraceptive is recommended. Consider therapy modification
Pitolisant: May decrease the serum concentration of Hormonal Contraceptives. Management: Patients using hormonal contraception should be advised to use an alternative non-hormonal contraceptive method during treatment with pitolisant and for at least 21 days after discontinuation of pitolisant treatment. Consider therapy modification
Pomalidomide: Progestins may enhance the thrombogenic effect of Pomalidomide. Management: Canadian pomalidomide labeling recommends caution with use of hormone replacement therapy and states that hormonal contraceptives are not recommended. US pomalidomide labeling does not contain these specific recommendations. Consider therapy modification
Primidone: May diminish the therapeutic effect of Progestins (Contraceptive). Contraceptive failure is possible. Management: Use of alternative, nonhormonal contraceptives is recommended. Consider therapy modification
Retinoic Acid Derivatives: May diminish the therapeutic effect of Progestins (Contraceptive). Retinoic Acid Derivatives may decrease the serum concentration of Progestins (Contraceptive). Management: Two forms of effective contraception should be used in patients receiving retinoic acid derivatives. Microdosed progesterone-only preparations (ie, minipills that do not contain estrogen) are considered an inadequate method of contraception. Exceptions: Adapalene; Alitretinoin (Topical); Bexarotene (Topical); Tretinoin (Topical). Consider therapy modification
Rifamycin Derivatives: May decrease the serum concentration of Progestins (Contraceptive). Contraceptive failure is possible. Management: Contraceptive failure is possible. Use of an alternative, nonhormonal contraceptive is recommended. Consider therapy modification
Saquinavir: May decrease the serum concentration of Progestins (Contraceptive). Management: Use an alternative or additional method of contraception due to possibly decreased contraceptive effectiveness. Injected depot medroxyprogesterone acetate does not appear to participate in this interaction. Consider therapy modification
Sarilumab: May decrease the serum concentration of CYP3A4 Substrates (High risk with Inducers). Monitor therapy
Selegiline: Progestins (Contraceptive) may increase the serum concentration of Selegiline. Monitor therapy
Siltuximab: May decrease the serum concentration of CYP3A4 Substrates (High risk with Inducers). Monitor therapy
St John's Wort: May diminish the therapeutic effect of Progestins (Contraceptive). Contraceptive failure is possible. Management: Consider using a product other than St John's wort. Contraceptive failure is possible. Use of an alternative, nonhormonal contraceptive is recommended. Consider therapy modification
Sugammadex: May decrease the serum concentration of Progestins (Contraceptive). Management: Patients receiving any hormonal contraceptive (oral or non-oral) should use an additional, nonhormonal contraceptive method during and for 7 days following sugammadex treatment. Consider therapy modification
Tazemetostat: May decrease the serum concentration of Hormonal Contraceptives. Management: Women of reproductive potential should use a non-hormonal contraceptive method during treatment with tazemetostat and for 6 months after. Men with female partners should use contraception during treatment and for 3 months after. Consider therapy modification
Tetrahydrocannabinol and Cannabidiol: May decrease the serum concentration of Hormonal Contraceptives. Management: Women using hormonal contraceptives should consider adding a barrier contraceptive due to the potential for tetrahydrocannabinol and cannabidiol to decrease concentrations and effectiveness of hormonal contraceptives. Consider therapy modification
Thalidomide: Progestins (Contraceptive) may enhance the thrombogenic effect of Thalidomide. Monitor therapy
Tipranavir: May increase the serum concentration of Progestins (Contraceptive). Management: Use an alternative or additional method of contraception due to possibly decreased contraceptive effectiveness. Injected depot medroxyprogesterone acetate does not appear to participate in this interaction. Consider therapy modification
Tocilizumab: May decrease the serum concentration of CYP3A4 Substrates (High risk with Inducers). Monitor therapy
Topiramate: May decrease the serum concentration of Progestins (Contraceptive). Management: Caution patients that this combination may be associated with reduced contraceptive effectiveness. Consider adding an additional (non-hormonal) contraceptive method. Consider therapy modification
Tranexamic Acid: Progestins (Contraceptive) may enhance the thrombogenic effect of Tranexamic Acid. Avoid combination
Triazolam: Hormonal Contraceptives may increase the serum concentration of Triazolam. Monitor therapy
Ulipristal: Progestins may diminish the therapeutic effect of Ulipristal. Ulipristal may diminish the therapeutic effect of Progestins. Management: Ulipristal for uterine fibroids (Canadian indication): avoid progestins within 12 days of stopping ulipristal; as emergency contraceptive (U.S. indication): avoid progestins within 5 days of stopping ulipristal. Avoid combination
Vitamin K Antagonists (eg, warfarin): Progestins (Contraceptive) may diminish the anticoagulant effect of Vitamin K Antagonists. In contrast, enhanced anticoagulant effects have also been noted with some products. Management: When possible, concomitant hormonal contraceptives and coumarin derivatives should be avoided in order to eliminate the risk of thromboembolic disorders. Consider using an alternative, nonhormonal contraceptive. Consider therapy modification
Voriconazole: May increase the serum concentration of Progestins (Contraceptive). Progestins (Contraceptive) may increase the serum concentration of Voriconazole. Monitor therapy
Adverse Reactions
Adverse effects as reported with any dosage form.
>10%:
Central nervous system: Headache (9% to 17%), nervousness (11%)
Endocrine & metabolic: Amenorrhea (IM: 55% at 12 months; 68% at 24 months; SubQ: 6%), weight gain (IM: >10 lbs at 24 months: 38%; SubQ: 6%), menstrual disease (IM: 57% at 12 months; 32% at 24 months; SubQ: 1% to 7%)
Gastrointestinal: Abdominal pain (1% to 11%)
1% to 10%:
Cardiovascular: Edema (2%)
Central nervous system: Dizziness (1% to 6%), anxiety (1% to <5%), depression (1% to <5%), insomnia (1% to <5%), irritability (1% to <5%), fatigue (<5%)
Dermatologic: Acne vulgaris (1% to <5%), alopecia (1%), skin rash (1%)
Endocrine & metabolic: Decreased libido (1% to 6%), change in menstrual flow (menometrorrhagia; 1% to <5%), hypermenorrhea (1% to <5%), hot flash (1% to <5%)
Gastrointestinal: Abdominal distension (1% to <5%), diarrhea (1% to <5%), nausea (1% to <5%), bloating (2%)
Genitourinary: Abnormal Pap smear (1% to <5%), bacterial vaginosis (1% to <5%), breast tenderness (1% to <5%), dysmenorrhea (1% to <5%), mastalgia (1% to <5%), urinary tract infection (1% to <5%), uterine hemorrhage (1% to <5%), vaginal hemorrhage (1% to <5%), vaginitis (1% to <5%), vulvovaginal candidiasis (1% to <5%), leukorrhea (3%)
Infection: Influenza (1% to <5%)
Local: Pain at injection site (1% to <5%), atrophy at injection site (≤1%), induration at injection site (≤1%)
Neuromuscular & skeletal: Arthralgia (1% to <5%), back pain (1% to <5%), limb pain (1% to <5%), leg cramps (4%), weakness (≤4%)
Respiratory: Bronchitis (1% to <5%), nasopharyngitis (1% to <5%), pharyngitis (1% to <5%), sinusitis (1% to <5%), upper respiratory tract infection (1% to <5%)
Frequency not defined:
Central nervous system: Euphoria, malaise
Endocrine & metabolic: Cushing syndrome, hypercalcemia, lipodystrophy
Genitourinary: Breakthrough bleeding, spotting
Local: Injection site nodule, tenderness at injection site
<1%, postmarketing, and/or case reports: Anaphylaxis, anaphylactoid reaction, anemia, angioedema, anxiety, asthma, axillary swelling, Bell palsy, body odor, breast changes, cervical cancer, change in appetite, change in cervical erosion, change in cervical secretions, chest pain, chills, chloasma, cholestatic jaundice, decreased bone mineral density, decreased glucose tolerance, decreased lactation, deep vein thrombosis, delayed return to fertility, diaphoresis, drowsiness, dyspareunia, dyspnea, fever, galactorrhea, genitourinary infection, hematologic abnormality, hirsutism, hoarseness, hypersensitivity reaction, increased libido, increased thirst, jaundice, lump in breast, malignant neoplasm of breast, nipple bleeding, nipple discharge, oligomenorrhea, optic neuritis, osteoporosis, paralysis, paresthesia, pathological fracture due to osteoporosis, pruritus, pulmonary embolism, rectal hemorrhage, residual mass at injection site, retinal thrombosis, scleroderma, seizure, skin discoloration (melasma), skin discoloration at injection site, sterile abscess at injection site, syncope, tachycardia, thrombophlebitis, urticaria, uterine hyperplasia, vaginal cyst, varicose veins, weight loss, xeroderma
Warnings/Precautions
Concerns related to adverse effects:
- Adrenal suppression: May cause suppression of hypothalamic-pituitary-adrenal (HPA) axis, resulting in decreased plasma cortisol concentrations, decreased cortisol secretion, and low plasma ACTH concentrations. Cushingoid symptoms may occur.
- Anaphylaxis/hypersensitivity reactions: Anaphylaxis or anaphylactoid reactions have been reported with use of the injection; medication for the treatment of hypersensitivity reactions should be available for immediate use.
- Bone mineral density loss: [US Boxed Warning]: Prolonged use of medroxyprogesterone contraceptive injection may result in a loss of bone mineral density (BMD). It is not known if use during adolescence or early adulthood will decrease peak bone mass accretion or increase the risk for osteoporotic fractures later in life. Loss is related to the duration of use, may not be completely reversible on discontinuation of the drug, and incidence is not significantly different between the SubQ and IM dosage forms. The impact on peak bone mass in adolescents should be weighed against the potential for unintended pregnancies in treatment decision. Consider alternative contraceptive methods in patients at risk for osteoporosis (eg, metabolic bone disease, chronic alcohol and/or tobacco use, anorexia nervosa, strong family history of osteoporosis, chronic use of medications associated with osteoporosis such as anticonvulsants or corticosteroids). All patients should have adequate calcium and Vitamin D intake. Consider evaluating bone mineral density in patients receiving high doses of medroxyprogesterone for long term endometrial cancer.
- Breast cancer: [US Boxed Warning]: Based on data from the Women's Health Initiative (WHI) studies, an increased risk of invasive breast cancer was observed in postmenopausal women using conjugated estrogens (CE) in combination with medroxyprogesterone acetate (MPA). Observational studies noted this risk declines once therapy is discontinued. The WHI study did not observe an increased risk of invasive breast cancer in women with a hysterectomy using CE alone. Women who used depo-medroxyprogesterone within the previous 5 years and for a duration of 12 months or longer were found to have an increased risk of breast cancer. The risk of breast cancer in postmenopausal patients on hormone therapy may depend upon type of estrogen and/or progestin, dose, timing of therapy initiation, duration of therapy, route of administration, and individual patient characteristics (AACE/ACE [Cobin 2017]; NAMS 2017). Hormone therapy may be associated with increased breast density (NAMS 2017); an increase in abnormal mammogram findings requiring further evaluation has been reported with estrogen alone or in combination with progestin therapy. Estrogen use may lead to severe hypercalcemia in patients with breast cancer and bone metastases; discontinue estrogen if hypercalcemia occurs. Most products are contraindicated in patients with known or suspected breast cancer. Use of medroxyprogesterone for the treatment of endometrial carcinoma is not recommended in women with known or suspected breast cancer and women with a strong family history of breast cancer should be carefully monitored.
- Dementia: [US Boxed Warning]: Estrogens with or without progestin should not be used to prevent dementia. In the Women's Health Initiative Memory Study (WHIMS), an increased incidence of probable dementia was observed in women ≥65 years of age taking CE in combination with MPA. Because the WHI memory studies were conducted in women ≥65 years of age, it is unknown if these findings apply to younger postmenopausal women. However, hormone therapy is not recommended at any age to prevent or treat cognitive decline or dementia (AACE [Goodman 2011]; NAMS 2017).
- Ectopic pregnancy: When used for contraception, the possibility of ectopic pregnancy should be considered in patients with severe abdominal pain.
- Endometrial cancer: MPA is used to reduce the risk of endometrial hyperplasia in nonhysterectomized postmenopausal women receiving conjugated estrogens. The use of unopposed estrogen in women with a uterus is associated with an increased risk of endometrial cancer. The addition of a progestin to estrogen therapy may decrease the risk of endometrial hyperplasia, a precursor to endometrial cancer. Adequate diagnostic measures, including endometrial sampling if indicated, should be performed to rule out malignancy in postmenopausal women with undiagnosed abnormal vaginal bleeding. There is no evidence that the use of natural estrogens results in a different endometrial risk profile than synthetic estrogens at equivalent estrogen doses. The risk of endometrial cancer appears to be dose and duration dependent and may persist following discontinuation of therapy. The use of a progestin is not generally required when low doses of estrogen are used locally for vaginal atrophy, although long term data (>1 year) supporting this recommendation are lacking (NAMS 2013; NAMS 2017).
- Hypertriglyceridemia: In women using estrogen plus progesterone therapy, triglycerides may be increased in women with preexisting hypertriglyceridemia; discontinue if pancreatitis occurs.
- Ovarian cancer: Available information related to the use of menopausal estrogen or estrogen/progestin therapy and risk of ovarian cancer is inconsistent. If an association is present, the absolute risk is likely rare and may be influenced by duration of therapy (AACE [Goodman 2011]; ES [Stuenkel 2015]; NAMS 2017).
- Retinal vascular thrombosis: Discontinue pending examination in cases of sudden partial or complete vision loss, sudden onset of proptosis, diplopia, or migraine; discontinue permanently if papilledema or retinal vascular lesions are observed on examination.
- Vaginal bleeding: Unscheduled bleeding/spotting may occur. Presentation of irregular, unresolving vaginal bleeding following previously regular cycles warrants further evaluation including endometrial sampling, if indicated, to rule out malignancy.
- Weight gain: Contraceptive therapy with medroxyprogesterone commonly results in an average weight gain of ~3.7 kg after 2 years of treatment.
Disease-related concerns:
- Abnormal uterine bleeding: When considering specific treatment for acute or chronic abnormal uterine bleeding (AUB) due to ovulatory dysfunction (not structural causes), consideration should be given to medical contraindications to available therapies as well as if simultaneous contraception is needed or pregnancy is desired (ACOG 136 2013; ACOG 557 2013).
- Asthma: Use estrogen plus progestin therapy with caution in patients with asthma; may exacerbate disease.
- Cardiovascular disease: [US Boxed Warning]: Estrogens with progestin should not be used to prevent cardiovascular disease. Using data from the Women’s Health Initiative (WHI) studies, an increased risk of deep vein thrombosis (DVT), pulmonary emboli (PE), and stroke has been reported with CE 0.625 mg with MPA 2.5 mg in postmenopausal women 50 to 79 years. Additional risk factors include diabetes mellitus, hypercholesterolemia, hypertension, SLE, obesity, tobacco use, and/or history of venous thromboembolism (VTE). Risk factors should be managed appropriately; discontinue use immediately if adverse cardiovascular events occur or are suspected. Use may be contraindicated in women with active DVT, PE, arterial thromboembolic disease (stroke and MI), or a history of these conditions. When used for contraception, use caution in patients with risk factors for cardiovascular disease (Curtis 2016b). If thrombosis develops with contraceptive treatment, discontinue treatment (unless no other acceptable contraceptive alternative).
- Depression: Use with caution in patients with a history of depression.
- Diabetes: Estrogen plus progestin therapy may have adverse effects on glucose tolerance; use caution in women with diabetes mellitus.
- Diseases exacerbated by fluid retention: Use with caution in patients with diseases which may be exacerbated by fluid retention, including cardiac or renal dysfunction.
- Epilepsy: Use estrogen plus progestin therapy with caution in patients with epilepsy; may exacerbate disease.
- Hepatic dysfunction: Estrogens plus progestins are poorly metabolized in patients with hepatic dysfunction. Use caution with a history of cholestatic jaundice associated with prior estrogen use or pregnancy. Discontinue if jaundice develops or if acute or chronic hepatic disturbances occur. Most products are contraindicated with hepatic impairment or disease. Use of medroxyprogesterone for the treatment of endometrial carcinoma is not recommended in women with significant hepatic dysfunction and should be discontinued if liver dysfunction occurs.
- Hepatic hemangiomas: Use estrogen plus progestin therapy with caution in patients with hepatic hemangiomas; may exacerbate disease.
- Hypoparathyroidism: Use estrogen plus progestin therapy with caution in patients with hypoparathyroidism; estrogen-induced hypocalcemia may occur.
- Migraine: Use caution in patients with migraine; may exacerbate disease.
- Porphyria: Use estrogen plus progestin therapy with caution in patients with porphyria; may exacerbate disease.
- Systemic lupus erythematosus: Use estrogen plus progestin therapy with caution in patients with systemic lupus erythematosus (SLE); may exacerbate disease.
Concurrent drug therapy issues:
- Drug-drug interactions: Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information.
Special populations:
- Menopause: Use may mask the onset of menopause in women treated for endometrial cancer.
- Pediatric: Not for use prior to menarche.
- Surgical patients: Whenever possible, progestins in combination with estrogens should be discontinued at least 4 to 6 weeks prior to surgery associated with an increased risk of thromboembolism or during periods of prolonged immobilization.
Dosage form specific issues:
- Polysorbate 80: Some dosage forms may contain polysorbate 80 (also known as Tweens). Hypersensitivity reactions, usually a delayed reaction, have been reported following exposure to pharmaceutical products containing polysorbate 80 in certain individuals (Isaksson 2002; Lucente 2000; Shelley, 1995). Thrombocytopenia, ascites, pulmonary deterioration, and renal and hepatic failure have been reported in premature neonates after receiving parenteral products containing polysorbate 80 (Alade 1986; CDC 1984). See manufacturer's labeling.
Other warnings/precautions:
- HIV infection protection: [US Boxed Warning]: Inform patients that injectable contraceptives do not protect against HIV infection or other sexually transmitted diseases. Women at high risk for HIV infection should be informed that there may be an increased risk of acquiring HIV with use of a progestin-only injection contraceptive. However, available data are inconsistent, and benefits of use may outweigh potential risk; treatment should not be withheld when appropriate. Women should be instructed about HIV prevention measures (Tepper 2017).
- Laboratory changes: The use of estrogens and/or progestins may change the results of some laboratory tests (eg, coagulation factors, lipids, glucose tolerance, binding proteins). The dose, route, and the specific estrogen/progestin influences these changes.
- Long-term use: [US Boxed Warning]: Long-term use (ie, >2 years) should be limited to situations where other birth control methods are inadequate. When used for endometrial carcinoma, the effects of long term use on adrenal, hepatic, ovarian, pituitary, and uterine function is not known.
- Risks vs benefits: When used for the relief of menopausal symptoms, the benefit-risk of combination hormone therapy is most favorable if started in patients who have no contraindications to therapy, are <60 years of age, within 10 years of menopause onset, have a favorable lipid profile, and do not have the factor V Leiden genotype or metabolic syndrome. Risk factors for cardiovascular disease should also be considered when evaluating therapy and route of administration (AACE/ACE [Cobin 2017]; NAMS 2017). [US Boxed Warning]: Estrogens with progestin should be used for the shortest duration possible at the lowest effective dose consistent with treatment goals and risks for the individual woman. Patients should be reevaluated as clinically appropriate to determine if treatment is still necessary. Available data related to treatment risks are from Women’s Health Initiative (WHI) studies, which evaluated oral CE 0.625 mg with or without MPA 2.5 mg relative to placebo in postmenopausal women. Other combinations and dosage forms of estrogens and progestins were not studied. Outcomes reported from clinical trials using CE with or without MPA should be assumed to be similar for other doses and other dosage forms of estrogens and progestins until comparable data becomes available.
Monitoring Parameters
Contraception: Assessment of pregnancy status (prior to therapy); weight (optional; BMI at baseline may be helpful to monitor changes during therapy); assess potential health status changes at routine visits (Curtis 2016a). BMD with long-term use (per manufacturer).
Endometrial cancer: Consider BMD with long term use; breast cancer (in women with a strong family history of breast cancer).
Endometrial hyperplasia, treatment (off-label use): Endometrial sampling every 3 to 6 months, although most appropriate frequency has not been determined (ACOG 631 2015; Trimble 2012)
Menopause: Prior to combination hormonal therapy, baseline risk for breast cancer and CVD. During therapy, age appropriate breast and pelvic exams; blood pressure; unscheduled bleeding lasting >6 months for endometrial pathology (sooner in patients who are obese, diabetic, or have a history of endometrial cancer); serum triglycerides (2 weeks after starting therapy in patients with baseline level >200 mg/dL); TSH (6 to 12 weeks after starting oral therapy in patients taking thyroid replacement); efficacy beginning 1 to 3 months after starting therapy, then every 6 to 12 months as appropriate. Duration of treatment should be evaluated at least annually (ES [Stuenkel 2015]).
Treatment of paraphilia/hypersexuality (Guay 2009; Reilly, 2000): Hepatic function test (baseline and during treatment if suspected hepatotoxicity); CBC (baseline); serum testosterone (baseline then monthly for 4 months then every 6 months); serum LH and prolactin (baseline and every 6 months); FSH (baseline); glucose; bone scan (baseline then annually) if serum testosterone significantly suppressed; gallbladder function; blood pressure; weight gain
Pregnancy
Pregnancy Considerations
Most products are contraindicated in women who are pregnant, suspected to be pregnant or as a diagnostic test for pregnancy.
In general, there is not an increased risk of birth defects following inadvertent use of the injectable medroxyprogesterone acetate (MPA) contraceptives early in pregnancy. Hypospadias has been reported in male babies and clitoral enlargement and labial fusion have been reported in female babies exposed to MPA during the first trimester of pregnancy. Ectopic pregnancies have been reported with use of the MPA contraceptive injection.
High doses impair fertility. [US Boxed Warning]: Medroxyprogesterone contraceptive should not be used as a long-term birth control method (ie, longer than 2 years) unless other birth control methods are considered inadequate.
Median time to conception/return to ovulation following discontinuation of MPA contraceptive injection is 10 months following the last injection and is unrelated to the duration of use.
Patient Education
What is this drug used for?
- It is used to prevent pregnancy.
- It is used to lower the chance of endometrial changes in women after change of life who are getting estrogen therapy.
- It is used to treat pain caused by endometriosis.
- It is used to treat uterine bleeding due to hormonal imbalance.
- It is used to treat endometrial cancer.
- It is used to treat kidney cancer.
- It is used to treat females who do not have a monthly period cycle.
- It may be given to you for other reasons. Talk with the doctor.
Frequently reported side effects of this drug
- Weight gain
- Dizziness
- Fatigue
- Nausea
- Vomiting
- Weight loss
- Anxiety
- Abdominal cramps
- Bloating
- Sex drive changes
- Acne
- Hair loss
- Hair growth
- Trouble sleeping
- Loss of strength and energy
- Enlarged breasts
- Tender breasts
- Leg cramps
- Joint pain
- Dark patches on face
- Menstrual changes
Other side effects of this drug: Talk with your doctor right away if you have any of these signs of:
- Liver problems like dark urine, fatigue, lack of appetite, nausea, abdominal pain, light-colored stools, vomiting, or yellow skin
- Cushing syndrome like weight gain in upper back or abdomen; moon face; severe headache; or slow healing
- Adrenal gland problems like severe nausea, vomiting, severe dizziness, passing out, muscle weakness, severe fatigue, mood changes, lack of appetite, or weight loss
- Severe cerebrovascular disease like change in strength on one side is greater than the other, trouble speaking or thinking, change in balance, or vision changes
- High calcium like weakness, confusion, fatigue, headache, nausea and vomiting, constipation, or bone pain
- Gallstones like pain in the upper right abdominal area, right shoulder area, or between the shoulder blades; yellow skin; or fever with chills
- Pancreatitis like severe abdominal pain, severe back pain, severe nausea, or vomiting
- Low calcium like muscle cramps or spasms, numbness and tingling, or seizures
- Blood clots like numbness or weakness on one side of the body; pain, redness, tenderness, warmth, or swelling in the arms or legs; change in color of an arm or leg; chest pain; shortness of breath; fast heartbeat; or coughing up blood
- Severe headache
- Severe abdominal pain
- Bulging eyes
- Vision changes
- Blindness
- Contact lens discomfort
- Breast soreness or pain
- Lump in breast
- Nipple discharge
- Vaginal pain, itching, and discharge
- Abnormal vaginal bleeding
- Depression
- Swelling
- Mood changes
- Trouble with memory
- Confusion
- Seizures
- Severe injection site irritation
- Signs of a significant reaction like wheezing; chest tightness; fever; itching; bad cough; blue skin color; seizures; or swelling of face, lips, tongue, or throat.
Note: This is not a comprehensive list of all side effects. Talk to your doctor if you have questions.
Consumer Information Use and Disclaimer: This information should not be used to decide whether or not to take this medicine or any other medicine. Only the healthcare provider has the knowledge and training to decide which medicines are right for a specific patient. This information does not endorse any medicine as safe, effective, or approved for treating any patient or health condition. This is only a brief summary of general information about this medicine. It does NOT include all information about the possible uses, directions, warnings, precautions, interactions, adverse effects, or risks that may apply to this medicine. This information is not specific medical advice and does not replace information you receive from the healthcare provider. You must talk with the healthcare provider for complete information about the risks and benefits of using this medicine.